In Summary
- A tumor is any abnormal mass of tissue formed by excessive cell proliferation; the word “cancer” refers specifically to malignant tumors that have acquired the capacity to invade adjacent tissue and metastasize.
- The critical biological distinction between benign and malignant tumors is not growth rate or size — it is the cellular loss of differentiation and the acquisition of invasive behavior, both driven by accumulated genomic instability.
- Most people who receive a “tumor” diagnosis without further qualification are experiencing fear calibrated to the wrong threat — the majority of tumors encountered incidentally are benign and clinically inconsequential.
- Understanding what makes a tumor malignant clarifies what prevention actually targets: not preventing abnormal cells from appearing, but preventing them from losing the constraints that keep them benign.
Of the questions patients bring to my clinic, few carry more emotional weight than: “Is it cancer?” And yet the question itself contains a conceptual confusion that makes it harder to answer clearly than it should be. The words “tumor” and “cancer” are used interchangeably in everyday language but mean quite different things biologically — and the difference matters enormously for prognosis, treatment, and, most practically, for how frightened a patient should be.
Let me explain what these terms actually mean from a pathology perspective, because the biology here is genuinely important and not well communicated in most clinical encounters.
What a Tumor Is
A tumor — from the Latin tumor, meaning swelling — refers to any abnormal mass of tissue that forms as a result of excessive cellular proliferation. This proliferation occurs when cells escape the normal regulatory mechanisms that constrain cell division: they continue to divide beyond the normal checkpoints that would trigger cell cycle arrest or apoptosis.
Tumors are classified into two fundamental categories: benign and malignant.
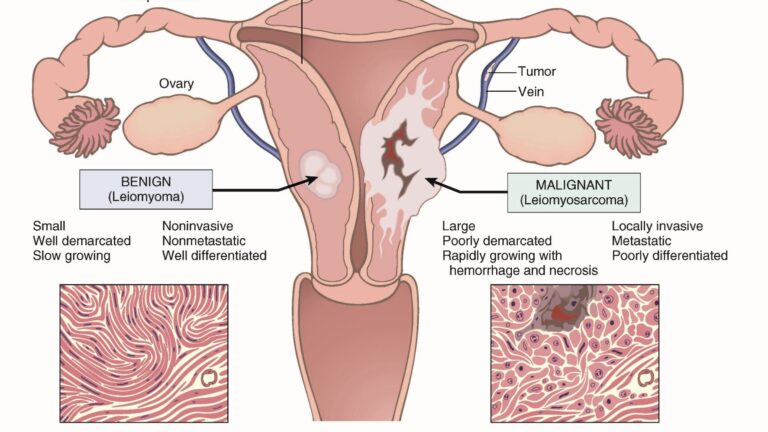
A benign tumor grows abnormally but respects the boundaries of the tissue in which it originates. Its cells remain well-differentiated — they retain the structural and functional characteristics of the tissue type they came from. A benign fat cell tumor (lipoma) still looks and behaves like a fat cell. Benign tumors are typically encapsulated, do not invade adjacent tissue, and do not spread to distant sites. They can be clinically significant if they grow large enough to compress adjacent structures, but they are not cancer.
A malignant tumor — which is what “cancer” means — is something fundamentally different. Malignant cells have lost the differentiation that kept their benign counterparts recognizable and contained. They no longer reliably perform the function of their tissue of origin. And critically, they have acquired the capacity to invade: to break through the basement membrane that defines their tissue boundary, to penetrate vascular and lymphatic channels, and to establish secondary colonies in distant organs — the process called metastasis.
It is this combination — loss of differentiation, invasive capacity, and metastatic potential — that defines malignancy. Not growth rate alone, and not size.
The Pathological Mechanism: What Goes Wrong
Understanding what makes a cell malignant requires understanding the normal constraints on cell behavior and what happens when those constraints fail.
In normal tissue, cell division is tightly regulated by the balance of proto-oncogenes (which promote cell division) and tumor suppressor genes (which constrain it). DNA repair mechanisms correct replication errors before they become permanent mutations. When damage exceeds repairability, apoptotic pathways eliminate the damaged cell before it can pass its errors to daughter cells. The entire system is redundant — multiple independent checkpoints must fail before a cell can pursue unconstrained proliferation.
Carcinogenesis — the development of cancer — is a multi-step process of accumulated failure in these systems. The current model holds that a minimum of five to ten driver mutations in critical regulatory genes are required before a cell achieves full malignant transformation. These mutations accumulate over years or decades, which is why cancer incidence rises steeply with age and why lifestyle factors that accelerate mutation accumulation or impair surveillance have such large effects on lifetime cancer risk.
The progression from normal cell to malignant cell typically passes through an intermediate state: dysplasia — abnormal cell morphology without yet crossing the threshold of invasiveness. Dysplastic cells are abnormal and represent genuine risk, but they have not yet become cancer. This intermediate state is the window in which intervention can prevent progression.
Why the Distinction Matters Clinically
The conflation of “tumor” with “cancer” causes significant clinical harm. Patients who receive an incidental finding of a benign tumor — a lipoma, a uterine fibroid, a thyroid nodule — and are not clearly told that benign means non-malignant experience fear calibrated to a threat that does not exist. This fear is itself clinically consequential: it drives overtreatment, unnecessary procedures, and the chronic psychological stress that, as I have written elsewhere, has its own adverse metabolic effects.
Conversely, understanding that cancer is a specific biological state — defined by invasiveness, not merely by abnormal growth — clarifies what treatment and prevention are actually targeting. Surgical removal of a well-encapsulated benign tumor is curative by definition: there is nothing left to spread. Treatment of malignancy must contend with the possibility that cells have already crossed tissue boundaries before detection, which is why systemic treatment considerations become relevant and why staging — assessing the extent of invasion and metastatic spread — is the first critical step after a malignant diagnosis.
The Korean Medicine Parallel
Classical Korean and Chinese medicine did not have a microscopic understanding of cellular biology, but they developed a clinical concept that maps meaningfully onto the benign-malignant distinction. The classical term for what we would recognize as malignant tumor — zheng jia (癥瘕) in Chinese, with related Korean terminology — distinguished between accumulations that were fixed, hard, and immovable (corresponding closely to what we would now identify as malignant, with the stromal invasion that makes malignant tumors adherent) and those that were movable, soft, and intermittent (corresponding to benign or functional masses).
The fixed, hard accumulation was understood as a consequence of severe Qi and Blood stagnation — a long-standing obstruction of normal circulation that had progressed to the point of structural consolidation. Treatment aimed at resolving the underlying stagnation, dispersing the accumulation, and restoring circulation. The logic was not incompatible with the modern understanding of the tumor microenvironment, in which dense stromal tissue and impaired vascularity contribute directly to treatment resistance.
Both traditions, from entirely different starting points, converge on a similar practical insight: the conditions that allow malignancy to establish and persist are not sudden events. They are the result of long-standing patterns — of metabolic environment, of immune function, of tissue homeostasis — that have been deteriorating for years before the first malignant cell appears.
Prevention, in both frameworks, means maintaining the conditions in which those deteriorating patterns do not progress to the point of no return.
This article reflects the clinical observations and teaching practice of Professor Seungho Baek, Professor of Korean Medicine at Dongguk University College of Korean Medicine, specializing in Pathology and Oncology.