In Summary
- Osteoporosis is not simply a calcium deficiency disease — it is a failure of bone remodeling dynamics in which resorption chronically outpaces formation, largely independent of calcium intake.
- The most powerful modifiable lever for preserving bone mass is mechanical loading through physical activity; calcium supplementation without this stimulus has limited effect on trabecular architecture.
- Korean medicine has long understood bone health as fundamentally a function of Kidney Jing — the constitutional essence that governs skeletal integrity — which helps explain why bone loss accelerates in states of constitutional depletion rather than dietary deficiency alone.
- The practical implication is counterintuitive: to protect bones, address the systemic depletion state as well as the local calcium economy — while keeping diagnosed osteoporosis under proper medical care.
Osteoporosis is one of the conditions that reveals most clearly the limitations of a purely biochemical model of disease. The standard clinical narrative — bones lose calcium, so supplement calcium — is not wrong exactly. It is just far downstream of where the problem actually originates, and treating it at that level alone produces correspondingly modest results.
Let me explain what is actually happening in bone tissue, and why the implications point toward a broader prevention strategy.
The Biology of Bone: A Dynamic System, Not a Static Structure
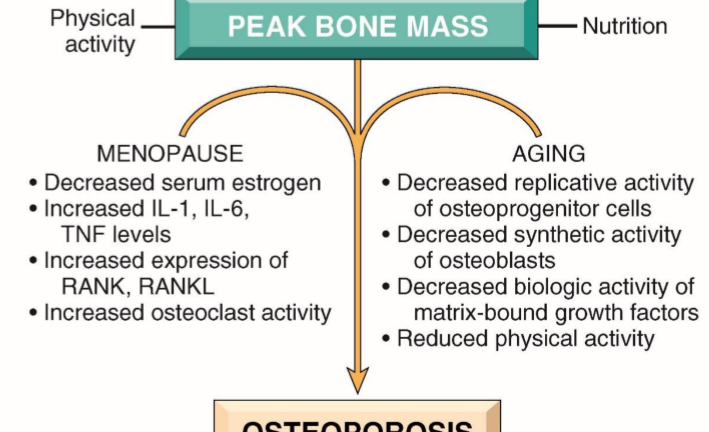
Bone is not inert mineral stored in a fixed structure. It is among the most metabolically active tissues in the body, continuously remodeled through the coordinated activity of two cell populations: osteoblasts, which synthesize new bone matrix, and osteoclasts, which resorb existing bone. In a healthy adult, these two processes are in dynamic equilibrium — bone is simultaneously being broken down and rebuilt, with the net result being maintained structural integrity.
Osteoporosis emerges when this equilibrium is disturbed — specifically when osteoclast activity chronically exceeds osteoblast activity, producing a net negative bone balance. The question is what disrupts this balance, and the answer is rarely a simple calcium shortage.
The primary regulators of osteoblast-osteoclast balance are hormonal and mechanical. On the hormonal side: estrogen, testosterone, parathyroid hormone, vitamin D, cortisol, and insulin-like growth factor-1 all exert significant influences on the relative activity of these two cell populations. On the mechanical side: physical loading through weight-bearing activity is the most potent physiological stimulus for osteoblast activation. Remove mechanical loading — as occurs during prolonged bed rest, zero-gravity exposure, or sedentary lifestyle — and osteoblast activity declines markedly regardless of calcium availability.
Why Calcium Supplementation Alone Is Insufficient
The calcium economy of bone is fundamentally a supply-and-demand story. Calcium is the raw material; osteoblast activity is the demand signal that determines whether and where that calcium is incorporated into bone matrix. Providing abundant calcium to an osteoblast-suppressed system is like supplying abundant building materials to a construction site where no workers have been scheduled.
The clinical trial evidence on calcium supplementation for osteoporosis prevention reflects this biology. Supplementation studies consistently show modest or inconsistent effects on bone density when evaluated in isolation. The studies that show the largest benefits are those in which calcium supplementation is combined with vitamin D (which enhances calcium absorption and has direct effects on bone cell differentiation) and with weight-bearing exercise (which provides the mechanical stimulus that calcium alone cannot substitute for).
The practical implication is important: patients who focus primarily on calcium intake while remaining sedentary are not addressing the primary driver of their bone loss. They are managing the raw material supply while ignoring the reason the material is not being used.
The Korean Medicine Framework: Kidney Jing and Bone Integrity
Korean medicine locates bone health within the Kidney organ system — not the anatomical kidneys specifically, but the constitutional framework that the Kidney system governs: the body’s fundamental reserve of inherited and acquired essence (Jing), which is the substrate for bone marrow production, hormonal synthesis, and the cellular regenerative capacity of bone-forming tissue. The classical principle is direct: the Kidney governs the bones.
This mapping is not merely metaphorical. The modern understanding of bone biology supports it closely. The hormones whose decline drives post-menopausal and age-related osteoporosis — estrogen, testosterone, growth hormone, IGF-1 — are precisely the hormones that Korean medicine would classify as expressions of Kidney Jing. The constitutional depletion patterns that Korean medicine identifies as Kidney deficiency — fatigue, low back weakness, declining reproductive function, premature aging, hair and tooth changes — are clinically associated with the same hormonal decline that drives bone loss.
The Korean medicine perspective adds a dimension the biochemical model tends to miss: bone loss is a systemic constitutional depletion event, not only a local calcium problem. The bones reflect the state of the entire body’s regenerative reserves. When those reserves are depleted — through chronic overwork, insufficient sleep, sustained constitutional overexertion, prolonged psychological stress, or the natural attrition of aging without adequate restoration — bone loss is one of the downstream consequences.
Prevention at the Right Level
Effective osteoporosis prevention operates at several levels simultaneously, and the further upstream the intervention, the greater its leverage.
At the most downstream level: calcium and vitamin D adequacy, weight-bearing exercise, and minimizing unnecessary bone-depleting medications where clinically appropriate — a decision to make with the prescribing physician, never by stopping a medication on one’s own. These measures are necessary but not sufficient.
At the intermediate level: hormonal environment management. This includes addressing the post-menopausal estrogen decline that drives bone loss most dramatically in women, and the testosterone decline that contributes in men; managing the chronic cortisol elevation that promotes osteoclast activity and suppresses osteoblast function; and maintaining the insulin sensitivity that supports IGF-1 activity in bone tissue.
At the deepest level — the level that Korean medicine addresses most directly — is constitutional restoration. In patients with significant Kidney Jing deficiency, herbal support through tonifying formulas that address the underlying constitutional depletion may help shift the broader physiological environment in which bone remodeling occurs. This is not calcium replacement, and it is not a substitute for medical treatment of established disease. It is an attempt to address the systemic condition that contributes to bone loss in the first place.
A necessary caveat: diagnosed osteoporosis — and especially a high fracture risk or a history of fragility fracture — should be assessed and managed with a physician, who may recommend bone-density monitoring and proven pharmacologic treatment. The constitutional and lifestyle measures described here work best alongside that care, not in place of it.
The patients who age with the best skeletal integrity into their eighties are not, in my clinical observation, the ones who took the most calcium supplements. They are the ones who maintained physical activity throughout their lives, managed their stress, slept well, and did not exhaust their constitutional reserves through chronic depletion.
This article reflects the clinical observations and teaching practice of Professor Seungho Baek, Professor of Korean Medicine at Dongguk University College of Korean Medicine, specializing in Pathology and Oncology.